1. Treatment objectives and treatment options in EoE
The treatment objectives in eosinophilic oesophagitis (EoE) are to achieve histological remission and to improve or remit clinical symptoms. The consequences of this should be the prevention of complications such as food bolus impaction and/or severe, refractory clinical symptoms requiring endoscopic rescue for extraction or dilation, respectively.1
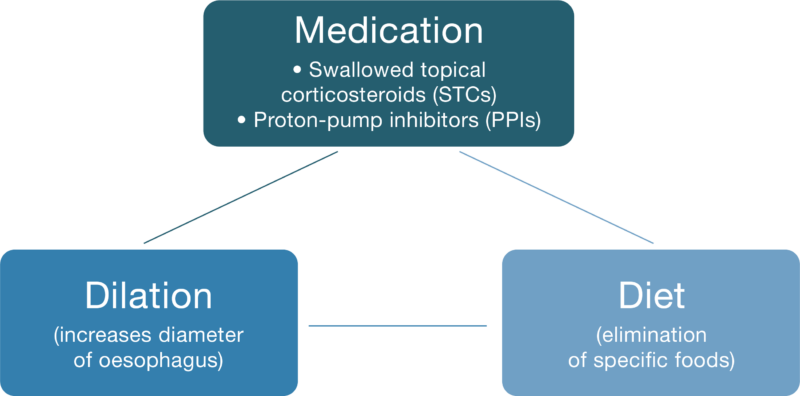
There are currently three different treatment options in EoE (see Fig. 1):
Medication (swallowed topical corticosteroids or proton-pump inhibitors)
Diets that eliminate specific foods to which the patient is allergic (i.e. foods are allergenic)
Endoscopic dilation of the oesophagus
Fig. 1: Treatment options in EoE.1
The different treatment options should be used based on the clinical presentation: Both the medications and elimination diets used in EoE have anti-inflammatory effects and directly impact on the underlying disease process. Endoscopic rescue may be required in cases of food bolus obstructions, which can't be self-cleared and/or to increase the diameter of the oesophagus (dilation). However, even accounting for the rapid symptom improvement as a common outcome with dilation, anti-inflammatory treatment should be ongoing in patients with EoE. This is because dilation of the oesophagus has no impact on the underlying disease.1
First-line treatment Medication (STCs or PPIs) or elimination diets are first-line treatment in adults with EoE. The treatment which is chosen should be based on the patient’s choice, in consultation with the treating physician, in addition to the experience of clinicians and available facilities where the patient is to be managed. As EoE is a chronic, progressive disease, once remission is achieved, maintenance treatment should be ongoing to avoid histological and thus clinical relapse. If this is not effectively controlled, it can lead to progressive inflammation and loss of function of the oesophagus associated with fibrosis and the consequences thereof, as detailed above.1,2
Need for long-term treatment EoE is a chronic, progressive inflammatory disease. It is currently not possible to cure EoE using either medication or elimination diets. When anti-inflammatory therapies are stopped, including after achieving significant improvement or even complete remission of symptoms, the inflammatory process in the oesophagus will quickly recommence, associated with histologic relapse (eosinophilia) and the consequential risk of fibrostenotic remodelling and worsening symptoms within a few weeks or months, which might become refractory to anti-inflammatory treatment. The risk of needing an endoscopy in an emergency department to extract food which has become lodged in patient’s oesophagus and/or to dilate the oesophagus is a potential consequence. Ongoing anti-inflammatory treatment is therefore critical, even when the EoE patient has only mild or no symptoms.1,3,4
2. Swallowed topical corticosteroids for the treatment of EoE
How effective are swallowed topical corticosteroids (STCs) in EoE patients? Until recently, STCs used in the treatment of EoE were repurposed asthma medications, which were swallowed rather than inhaled.1 Depending on the specific medication, it is either sprayed directly into the patient’s mouth, or first mixed with a viscous material like Splenda® or honey and then swallowed. A purpose-specific STC was recently approved in Australia for the treatment of EoE, which is a tablet which dissolves when placed on the patient’s tongue, thereby releasing the active ingredient (‘orally disintegrating’). The objective of all these treatments is to deliver sufficient drug concentrations efficiently to the lining of the oesophagus, where it is taken up to treat the pathology.5–8
Based on results from clinical studies, STCs are the most effective anti-inflammatory treatments for EoE, with histologic remission achieved in approximately 65% of patients with the repurposed asthma medications and over 90% with the orally disintegrating STC.8,9
What are the expected side effects/limitations when using topical corticosteroids in the oesophagus?
Importantly, the systemic absorption of these swallowed topical corticosteroids (STCs) is substantially lower than the systemic-acting steroids (e.g. prednisolone) and thus the risk of systemic adverse events is also substantially lower with STCs. As such, most of the side effects are localised, including mild fungal infections (candidiasis) of the mouth or oesophagus, which can occur in 10–15% of patients, easily treatable with an oral anti-fungal medication, without stopping the STC.6,11
3. Proton-pump inhibitors for the treatment of EoE
How effective are proton-pump inhibitors in treating EoE? Proton-pump inhibitors (PPIs), which are normally prescribed in treat gastro-oesophageal reflux (GORD), have also been used off-label to treat EoE, commonly at twice the recommended daily dose for GORD, as they appear to have an anti-inflammatory effect in these patients, independent of their acid suppression effects.1,4,12
In clinical studies in EoE patients, histologic and/or clinical remission rates of approximately 50% are achieved with PPIs.13
What are the expected side effects/limitations when using proton-pump inhibitors? PPI are considered relatively safe. The most-common side effects in EoE include headache, abdominal pain, constipation, diarrhoea, flatulence, nausea/vomiting and non-cancerous polyps in the stomach.14
4. Elimination diets in the treatment of EoE
Rationale for an elimination diet to treat EoE? Successful identification and elimination of the food(s) that trigger an allergic reaction in the oesophagus should have an anti-inflammatory effect. This is because the stimulus for the migration of eosinophils to the oesophageal mucosa would be prevented (or significantly reduced) and thus the primary mediator of the pathology in the oesophagus in EoE is removed, allowing the natural healing mechanisms to repair the damaged oesophagus, to return to a more normal state, associated with an improvement or remission of symptoms of dysfunction. This is the rationale for elimination diets as a treatment in EoE.12
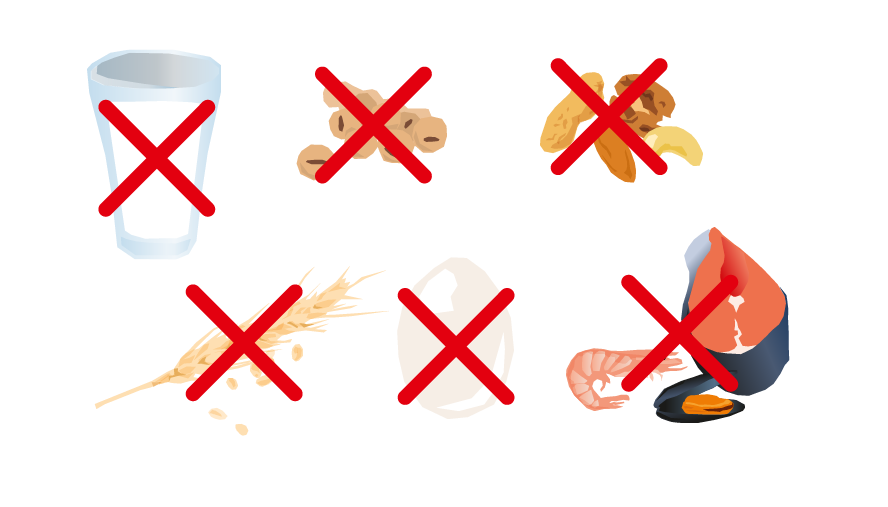
The foods that most commonly trigger inflammation in the oesophagus are dairy products, wheat, soy, nuts as well as fish/shellfish and legumes (see Fig. 2). As some EoE patients are allergic to multiple foods, a successful elimination diet can be highly restrictive.2,15
Fig. 2: Food allergens to be avoided during an identified elimination diet (animal milk and dairy products, soy/legumes, nuts, wheat, eggs, fish/shellfish).2,15
Empiric Elimination diet? The empiric elimination diet is the most widely used in adults with EoE, of which there are a few approaches; from the 6-food to the 2-food elimination (usually dairy and wheat) and the dairy-only elimination diet. In the 6-food diet, all 6 food groups are eliminated. After remission is achieved through this complete elimination (confirmed by endoscopy after 6 to 8 weeks), each food is then re-introduced into the diet, one by one, to determine if it causes a histologic relapse. If so, it is therefore identified as the food to which the patient is allergic and thus can be permanently eliminated from the patient’s diet. At this point, histologic remission needs to re-established (confirmed by endoscopy 6-8 weeks later) and a new food can be reintroduced, and procedure is repeated.2,15
Conversely, if the introduced food doesn’t cause a relapse, it is considered to be non-allergenic and can be maintained in the patient’s diet. Another of these 6 foods can then be immediately re-introduced to the patient’s diet.2,15
A similar approach is followed with the 2-food elimination or dairy-only elimination diet, albeit they are clearly easier to follow as less foods are involved. However, as would be anticipated, these latter diets are generally not as effective as the 6-food approach, owing to many EoE patients being allergic to multiple foods. This was confirmed across several clinical studies, with the 6-food elimination diet being effective (histologic remission) over a range of approximately 50–75% of patients, while the 4-food diet was effective over a range of approximately 55–65% of patients, with a single study reporting histologic remission in 43% of EoE patients receiving the 2-food elimination diet.15
A relatively recent approach to the 6 food diet involves a step-up approach (see Fig. 3) in which the 1–2 foods are eliminated first and then reintroduced, starting with the foods most likely to be allergenic (dairy & wheat) and then progressing stepwise to 4 and then 6 food elimination, based on the patient responses. This way not all 6 foods are eliminated at the beginning of the diet, as per the top-down approach described above, which is likely to be more acceptable to patients.4,15
Fig. 3: Step-up compared with top-down approach to elimination diets.15,16
What are the expected limitations with an empiric elimination diet?
It can take several months to identify all of the triggering foods, if the 6-food approach is employed. During this time, patients may need to undergo up to eight endoscopies to identify the allergic foods. Not only is this likely to be very onerous for the patient, the limited availability of endoscopy suites to conduct these procedures could be problematic – in addition to the associated expense – as could finding a dietitian with practical knowledge of EoE to oversee the patient’s diet.17–19
Furthermore, even if all the allergenic foods have been identified, the risk of ‘food contamination’ will always exist for a EoE patient when eating out or travelling unless they always prepare their own meals. This, plus the added expense of buying goods that are guaranteed to be free of the specific allergen(s) makes the long-term compliance of an elimination diet difficult and can lead to significant anxiety. In such a scenario, effective medication in a fully compliant individual might be a better option for an EoE patient as diet restrictions should not normally be required since any inflammatory response in the oesophagus following the exposure to the allergen(s) will be suppressed by these drugs.17–19
5. Endoscopic dilation for the treatment of EoE
What is the medical evidence for dilation? Dilation is commonly performed in patients with symptoms refractory to their anti-inflammatory fibrostenotic treatment and/or those at high risk of a food bolus obstruction due to significant remodelling in their oesophagus.17–19
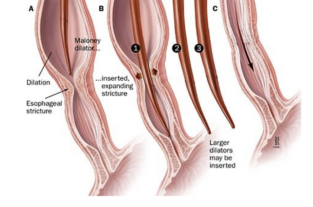
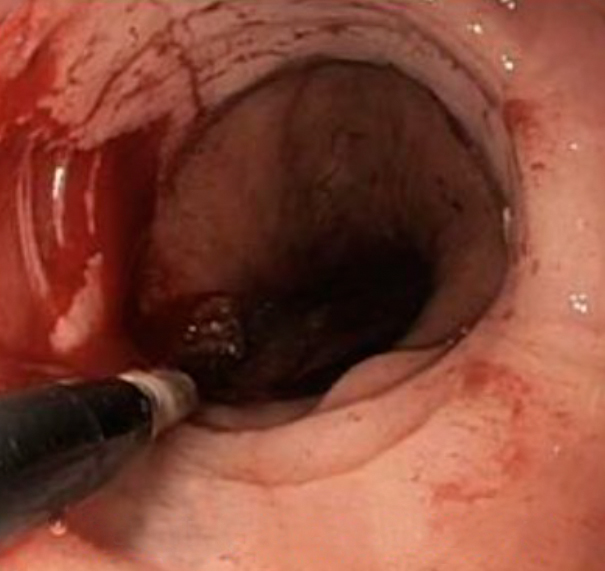
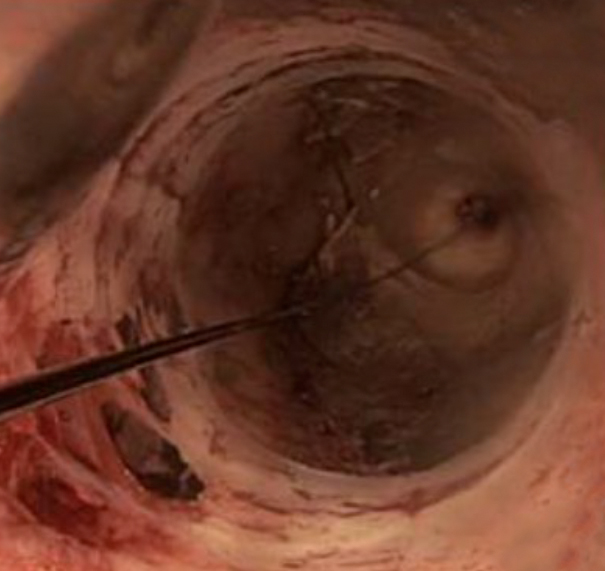
How is an oesophageal dilation performed? Should one or more strictures form, the diameter of the oesophagus can be widened through an endoscopic procedure. This is performed by expanding the area using either a balloon or long tube called a bougie. In the case of the former approach, an endoscopically passed balloon is inflated at the point of narrowing to a diameter large enough to cause significant stretch but not rupture. In contrast, the bougie approach involves passing a long tube set at a fixed diameter through the area being treated in order to stretch that area to the specific diameter, which is often the entire oesophagus. As strictures can be hard to detect on endoscopy, some gastroenterologists prefer bougies to increase the probability of treating all strictures; those seen as well as those unseen (Figs 4 and 5).20,21
Dilation takes about 10 minutes and is performed under sedation (see Figs. 4 and 5). Patients commonly experience rapid symptom relief, however, dilation does not treat the underlying pathology, meaning strictures may recur over time in the absence of effective anti-inflammatories and will require repeated dilation.20,21
What are the expected side effects/limitations when performing oesophageal dilation? Mild chest pain, normally transient, is a commonly reported post-procedure, which can be well managed using conventional pain medication. The risk of complications, particularly oesophageal perforation, is relatively low (<1%).20–22
6. References
Straumann A, Katzka DA. Diagnosis and treatment of eosinophilic oesophagitis. Gastroenterology 2018; 154(2):346– 59.
Arias Á, González-Cervera J, Tenías JM, Lucendo AJ. Efficacy of dietary interventions for inducing histologic remission in patients with eosinophilic oesophagitis: a systematic review and meta-analysis. Gastroenterology 2014; 146(7):1639–48.
Runge TM, Eluri S, Woosley JT, Shaheen NJ, Dellon ES. Control of inflammation decreases the need for subsequent esophageal dilation in patients with eosinophilic esophagitis. Dis Esophagus 2017;30(7):1–7.
Attwood S, Epstein J. Eosinophilic oesophagitis: recent advances and practical management. Frontline Gastroenterol 2020;12(7):644–9.
Dellon ES, Woosley JT, Arrington A, McGee SJ, Covington J et al. Efficacy of budesonide vs fluticasone for initial treatment or eosinophilic esophagitis in a randomized controlled trial. Gastroenterology 2019;157(1):65–73.e5.
Straumann A, Lucendo AJ, Miehlke S, Vieth M, Schlag C et al. Budesonide orodispersible tablets maintain remission in a randomized, placebo-controlled trial of patients with eosinophilic esophagitis. Gastroenterology 2020;159(5):1672–85.e5.
Therapeutic Goods Administration. JORVEZA budesonide 1 mg orally disintegrating tablet blister pack (322645). Available at: https://www.tga.gov.au/resources/artg/322645. Accessed March 2023.
Therapeutic Goods Administration. JORVEZA budesonide 0.5 mg orally disintegrating tablet blister pack (350996). Available at: https://www.tga.gov.au/resources/artg/350996. Accessed March 2023.
Rank MA, Sharaf RN, Furuta GT, Aceves SS, Greenhawt M et al. Technical review on the management of eosinophilic esophagitis: A report from the AGA Institute and the Joint Task Force on Allergy-Immunology Practice Parameters. Ann Allergy Asthma Immunol 2020;124(5):424–40.e17.
Lucendo AJ, Miehlke S, Schlag C, Vieth M, von Arnim U et al. Efficacy of budesonide orodispersible tablets as induction therapy for eosinophilic esophagitis in a randomized placebo-controlled trial. Gastroeneterology 2019;157(1):74–85.e15.
JORVEZA® (budesonide) orally disintegrating tablets Product Information, December 2021.
Carr S, Chan ES, Watson W. Correction to: Eosinophilic esophagitis. Allergy Asthma Clin Immunol 2019;15:22.
Lucendo AJ, Arias A, Molina-Infante J. Efficacy of proton pump inhibitor drugs for inducing clinical and histologic remission in patients with symptomatic esophageal eosinophilia: A systematic review and meta-analysis. Clin Gastroenterol Hepatol 2016;14(1):13–22.e1.
Gutiérrez-Junquera C, Fernández-Fernández S, Cilleruelo ML, Rayo A, Echeverría L et al. Long-term treatment with proton pump inhibitors is effective in children with eosinophilic esophagitis. J Pediatr Gastroenterol Nutr 2018;67(2):210–6.
Molina-Infante J, Arias Á, Alcedo J, Garcia-Romero R, Casabona-Frances S, Prieto-Garcia A et al. Step-up empiric elimination diet for pediatric and adult eosinophilic oesophagitis: The 2-4-6 study. J Allergy Clin Immunol 2018; 141(4):1365–72.
Votto M, De Filippo M, Lenti MV, Rossi CM, Di Sabatino A et al. Diet therapy in eosinophilic esophagitis. Focus on a personalized approach. Front Pediatr 2021;9:820192.
Zalewski A, Doerfler B, Krause A, Hirano I, Gonsalves N. Long-term outcomes of the six-food elimination diet and food reintroduction in a large cohort of adults with eosinophilic esophagitis. Am J Gastroenterol 2022;117(2):1963–70.
Philpott H, Nandurkar S, Royce SG, Thien F, Gibson PR. A prospective open clinical trial of a proton pump inhibitor, elimination diet and/or budesonide for eosinophilic oesophagitis. Aliment Pharmacol Ther 2016;43(9):985–93.
Wang R, Hirano I, Doerfler B, Zalewski A, Gonsalves N et al. Assessing adherence and barriers to long-term elimination diet therapy in adults with eosinophilic esophagitis. Dig Dis Sci 2018;63(7):1756–62.
Jung KW, Gundersen N, Kopacova J, Arora AS, Romero Y, Katzka D et al. Occurrence of and risk factors for complications after endoscopic dilation in eosinophilic oesophagitis. Gastrointest Endosc 2011; 73(1):15–21.
Sami SS, Haboubi HN, Ang Y, Boger P, Bhandari P. UK guidelines on oesophageal dilatation in clinical practice. Gut 2018;67(6):1000–23.
Lucendo AJ, Molina-Infante J. Esophageal dilation in eosinophilic esophagitis: risks, benefits, and when to do it. Curr Opin Gastroenterol 2018;34(4):226–32.